
From the 1Centre for Health Economics and Medicines Evaluation, School of Healthcare Sciences, Bangor University, Bangor, Gwynedd, 2North Wales Centre for Primary Care Research, Gwenfro Units 4–8, Wrexham Technology Park, Wrexham, 3Betsi Cadwaladr University Health Board, North Wales, Ysbyty Gwynedd, Penrhosgarnedd, Bangor, Gwynedd, and 4Department of Health Services Research, University of Liverpool, Liverpool, UK
Objective: As part of a wider feasibility study, the feasibility of gaining older patients’ views for hip fracture rehabilitation services was tested using a discrete choice experiment in a UK context.
Design: Discrete choice experiment is a method used for eliciting individuals’ preferences about goods and services.
Subjects/patients: The discrete choice experiment was administered to 41 participants who had experienced hip fracture (mean age 79.3 years; standard deviation (SD) 7.5 years), recruited from a larger feasibility study exploring a new multidisciplinary rehabilitation for hip fracture.
Methods: Attributes and levels for this discrete choice experiment were identified from a systematic review and focus groups. The questionnaire was administered at the 3-month follow-up.
Results: Participants indicated a significant preference for a fully-qualified physiotherapist or occupational therapist to deliver the rehabilitation sessions (β = 0·605, 95% confidence interval (95% CI) 0.462–0.879), and for their rehabilitation session to last less than 90 min (β = –0.192, 95% CI –0.381 to –0.051).
Conclusion: The design of the discrete choice experiment using attributes associated with service configuration could have the potential to inform service implementation, and assist rehabilitation service design that incorporates the preferences of patients.
Key words: discrete choice experiment; hip fracture; rehabilitation; service configuration; older people; activities of daily living.
Accepted Apr 4, 2018; Epub ahead of print May 14, 2018
J Rehabil Med 2018; 00: 00–00
Correspondence address: Joanna M. Charles, Centre for Health Economics and Medicines Evaluation, School of Healthcare Sciences, Bangor University, Bangor, Gwynedd, LL57 2PZ, UK. E-mail: j.charles@bangor.ac.uk
In this study, older patients who recently experienced hip fracture were asked to state their preferences about hip fracture services. A method used specifically for eliciting preferences, the discrete choice experiment, was used. Using a questionnaire, hypothetical services were presented to patients 3 months after their hip fracture, asking them to state which service they preferred. Older patients stated preferences for a fully-qualified physiotherapist or occupational therapist to deliver the rehabilitation sessions, and for their rehabilitation session to last less than 90 min. By asking about service structure (for example, where rehabilitation takes place and who will deliver the rehabilitation), a preferred package of rehabilitation could be offered to patients in future, aiding their recovery.
Hip fracture is a common health issue in older age, with consequences for the individual, such as mortality and loss of function. Approximately 70,000–75,000 hip fractures occur in the UK each year (1), and approximately a quarter of individuals who experience hip fracture die within the subsequent 12 months (2). The costs of hip fracture to UK publically funded health and social services are over £2 billion per annum (1). Multidisciplinary rehabilitation is one proposed method to help older people recover after a hip fracture (3); however, evidence as to the best way to deliver a rehabilitation service is inconclusive, and more research is required (4).
Discrete choice experiments (DCEs) are a stated preference technique for eliciting individuals’ preferences about goods and services (5, 6). DCE is based on the theory that individuals make trade-offs between choices (5, 6). These choices provide information about individuals’ relative preferences for different attributes of a service (5). In DCEs, a hypothetical good or service is presented based on a number of attributes (characteristics), each of which has differing levels. For example, the attribute “time” could have levels of 30, 60 and 90 min. These attributes and levels create choice sets. In a paired-choice DCE, as presented in this paper, in each scenario the respondent is asked to choose which service they prefer. The respondents were asked to pick “Service A” or “Service B”, based on the characteristics of the service presented (7). However, other DCE designs are available (for example, presenting current service configuration alongside the choice sets, or providing a “neither” option for the respondent’s preference). Published literature from Australia has explored hip fracture using DCEs assessing patients’ preferences regarding hip fracture rehabilitation (8, 9).
Milte et al. (8) explored what patients were willing to endure during rehabilitation in order to improve their mobility. Hypothetical scenarios were based on the attributes of: risk of falling; levels of pain; levels of physical effort; and mobility. Eighty-seven respondents, aged between 71 and 80 years, answered the DCE questionnaire. The results demonstrated that respondents expressed a strong preference for improvement in mobility and a willingness to participate in rehabilitation programmes involving moderate pain and effort.
The differences in preferences of patients and clinicians for rehabilitation service delivery in southern Australia have been studied by Laver et al. (9), who developed attributes based on characteristics of the service and individual characteristics. Hypothetical scenarios were based on the attributes of: mode of therapy; dose of therapy; team providing therapy; amount of recovery made; and cost of therapy programme. A total of 100 patients answered the DCE questionnaire, mean age 75 years, although only 15% of patients were receiving rehabilitation following a fall. Twenty-three occupational therapists and 91 other rehabilitation clinicians completed the DCE questionnaire. The results demonstrated that recovery was highly valued by both patients and clinicians, although higher doses of therapy (e.g. 6 h/day) were regarded as less acceptable. Clinicians were more accepting of new approaches (e.g. technology) and higher intensity therapies. Conversely, patients strongly valued more traditional, individualistic approaches.
Qualitative methods have also been employed to explore what is important to patients following hip fracture. Griffiths et al. (10) found that 4 months after hip fracture 31 UK patients, mean age 81.5 years, stated that stable mobility, particularly when performing valued activities (e.g. personal care, day-to-day activities and hobbies) was most important to them following hip fracture.
As rehabilitation after hip fracture is varied in the UK, with differing levels of services delivered in the community following discharge from hospital, it is important to understand preferences for services. This paper aims, for the first time in a UK context, to explore the feasibility of gathering older patients’ preferences for hip fracture rehabilitation services, as part of a larger feasibility study, the Fracture in the Elderly Multidisciplinary Rehabilitation (FEMuR) study (11). This method was chosen as it provides an indication of which characteristics are important to patients. Stated preference methods, such as DCES, can identify the trade-offs individuals make between the attributes presented. DCEs also provide a direction of preference; for example, DCEs are able to indicate if time is important to respondents and, importantly, whether it is more or less time spent performing supervised exercises they prefer.
The FEMuR feasibility study was designed to test an enhanced multidisciplinary rehabilitation intervention following hip fracture, comprising a patient-held information workbook, goal-setting diary and extra physiotherapy sessions in addition to usual care (11). The FEMuR study was conducted as a pragmatic randomized controlled feasibility trial with measures assessed at baseline and at 3-month follow-up (11). Participants were recruited from the 3 acute hospitals of Betsi Cadwaladr University Health Board (BCUHB) in North Wales (Wrexham Maelor, Ysbyty Glan Clwyd and Ysbyty Gwynedd) during the 6-month study period (11). The feasibility study recruited older adults recovering on an orthopaedic ward with proximal femoral fracture who were previously living independently and who had recently received surgical treatment. The specific inclusion and exclusion criteria are listed below.
As part of the FEMuR feasibility study, a DCE was designed to explore the feasibility of gathering older patients’ preferences for hip fracture rehabilitation services. The attributes and levels included in this DCE were identified from a systematic review, focus groups and a survey used to develop the FEMuR intervention (11). The focus groups were conducted with service users who had previously experienced hip fracture and rehabilitation services in the health board. Focus groups and a survey were also conducted with staff who deliver rehabilitation following hip fracture. These methods were employed, since different methods of attribute development can lead to different attribute choices and levels in the final DCE (6, 12). We sought published evidence and the opinions of both patients and healthcare professionals to develop a DCE that was relevant to patients, which produced attributes they considered to be important, but which was also grounded in “real-world” services, so that patients were presented with attributes of which they had experience. The main findings from each method were synthesized by the research team, who used common themes across all methods to arrive at a final set of attributes. Levels were chosen based on the principles of acceptability and plausibility (6).
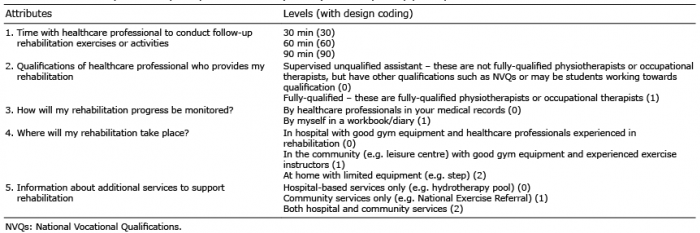
Table I describes the attributes and levels used in the DCE questionnaire. This list of attributes and levels yielded a total of 108 possible hypothetical scenarios. However, to create manageable number of scenarios for the participants with an efficient design, we used the appropriate mixed-level orthogonal arrays (13,14), which resulted in a reduced number of 16 pairwise choices with a total of 32 hypothetical scenarios, using a fold-over design. For each of the 16 pairwise choice tasks, participants were presented with 2 hypothetical rehabilitation service scenarios and asked to choose their preferred service, “A” or “B”.
Table I. Attributes and levels (and design coding) used in the discrete choice experiment (DCE) questionnaire administered to the Fracture in the Elderly Multidisciplinary Rehabilitation (FEMuR) feasibility study participants
An example of a DCE question presented to the participants in the feasibility study is provided in Fig. 1. Microsoft Word was used to create the DCE questionnaire, which was administered in English as a paper questionnaire. The DCE questionnaire was administered at the 3-month follow-up, with a researcher present to explain the questionnaire and answer any questions the participants may have had when completing the measure. The aim of the study was to test whether this DCE method was feasible for use with an older population. Ethical approval to undertake the DCE was granted by the UK NHS North Wales Research Ethics Committee – West (reference number 12/WA/0355).
Fig. 1. Example of a discrete choice experiment (DCE) question presented to participants in the feasibility study.
Random effects logit regression was used to analyse the data using STATA Version 10.1 (StataCorp, College Station, TX, USA) (6). This approach was chosen due to the forced choice design of DCE, which required respondents to choose between “Service A” or “Service B” (6).
U = βtime + βqualification + βmonitor + βplace + βinfo + ε
where: U = utility, βi = estimated coefficient for each attribute, and ε = error term.
All attributes containing more than 2 levels were effects coded in order to analyse individual levels in the random effects logit regression. Non-parametric 5,000 bootstrap replications were also conducted as part of the analyses to gain stability around the coefficient estimates, in order to create bootstrapped 95% confidence intervals. Tests for linearity were conducted by specifying a random effects regression model with the “time with healthcare professional” attribute using effects coding (15). Scale and preference heterogeneity was not explored in the analysis. A dominance test was not included, as none of the profiles generated by the design catalogue were dominant. An additional question to test for dominance was not added to the questionnaire, in order to administer the least burdensome questionnaire to participants. Due to the small sample size of this feasibility study, sub-group analyses were not possible.
During development of the DCE it was hypothesized that: participants would prefer more time with the healthcare professional; the sessions would be delivered by a fully-qualified physiotherapist or occupational therapist; participants would prefer to monitor their own progress using a workbook/diary; patients would prefer to undertake their rehabilitation at home; and patients would prefer information about additional services based in both hospital and the community to support their rehabilitation.
Of the 61 participants recruited to the feasibility trial, 9 withdrew, 4 were lost to follow-up, and 16 were non-completers. Thirty-two sets of questionnaires were available to analyse (representing 52% of the FEMuR study sample). Reasons for non-completion are described below.
One participant completed the follow-up assessment over the phone; therefore, the DCE could not be completed as the measure cannot be administered over the phone. One participant was given a previous version of the questionnaire, which had more than 16 scenario choice sets. Eight participants did not receive any rehabilitation, and therefore, felt the DCE questionnaire was not relevant to them and declined to complete it. Four participants struggled to understand the questionnaire and how to answer it; therefore, they did not complete the measure. Two participants left questions blank and, as the DCE questionnaire requires all questions to be answered in order to be analysed, these participants were removed from the final analysis. Hence, analysis was conducted on 32 participants after removing the 9 who withdrew, the 4 lost to follow up, and the 16 non-completers. Ryan et al. (6) suggest that a sample size of at least 30 individuals is required to undertake analysis; therefore, this pilot DCE analysed the results from the 32 sets of completed data received.
Table II describes the baseline characteristics of the DCE sample compared with the FEMuR feasibility study sample. Baseline characteristics described were obtained prior to randomization. There were more females than males in the DCE and the feasibility trial samples (22, 69%; 46, 75%, respectively), with an overall mean age of 79.3 years in the DCE sample and an overall mean age of 79.4 years in the feasibility study sample. Slightly more participants in the DCE sample lived with others (17, 53%) compared with the feasibility sample (30, 49%). In both the feasibility study and DCE samples, the majority of participants owned their own homes (48, 79%; 25, 78%, respectively), with fewer participants living in privately rented properties, housing association/local authority properties or sheltered accommodation. Hemi-arthoplasty surgery was the most common type of surgery received, followed by internal fixation in both the DCE sample (13, 41%; 11, 34%) and the feasibility study sample (29, 47%; 17, 28%). The majority of participants who completed the DCE questionnaire were recruited from Wrexham Maelor Hospital (16, 50%), and the least number of participants were recruited from Ysbyty Gwynedd (Gwynedd Hospital) (2, 6%). In comparison, the majority of participants for the feasibility study were recruited from Ysbyty Glan Clwyd (Glan Clwyd Hospital) (34, 56%), and the least number of participants were recruited from Ysbyty Gwynedd (Gwynedd Hospital) (11, 18%). The feasibility study (11) also gathered anonymized cohort data on 400 proximal hip fracture patients in North Wales. Comparisons of the 2 samples (cohort and feasibility study) found similarity in sex, type of hip fracture and type of hip surgery; although no formal tests for statistical significance were conducted (11). The only difference found was in age; with the cohort population being slightly older than the feasibility study sample, with a mean age difference of 4.5 years (11). Baker et al. (16) explored a cohort of 10,044 UK hip fracture patients using the Nottingham Hip Fracture Database. The feasibility study sample is similar to this larger cohort in terms of sex, type of hip fracture and type of hip surgery. The larger cohort reported an older median age of 82 years, a difference of 3 years compared with the feasibility study sample.
Table II. Discrete choice experiment (DCE) sample characteristics (n = 32)
Out of our FEMuR feasibility study sample of 61 older patients, 32 older patients (52%) were able to complete the DCE questionnaire. Fig. 2 shows plots of the estimated coefficients from the random effects logit regression for “time with the healthcare professional”. It can be seen from Fig. 2 that the attribute of “time with the healthcare professional” was not linear and therefore we analysed this as a categorical attribute.
Table III shows the results of the random effects logit regression. Only 2 attributes were statistically significant (p < 0.05). Participants indicated a significant preference for their rehabilitation to be delivered by a fully-qualified physiotherapist or occupational therapist, rather than a supervised unqualified physiotherapy or occupational therapy assistant. Participants also showed a significant preference for their rehabilitation session to last less than 90 min.
Table III. Results from the random effects logit regression model: discrete choice experiment (DCE) sample (n = 32)*a
This is the first DCE undertaken in the UK to investigate patients’ preferences for rehabilitation service configuration following hip fracture. The feasibility trial demonstrated that the DCE method could be used with elderly patients. Two attributes were found to be important to participants. Participants indicated a statistically significant preference for the healthcare professional delivering the rehabilitation sessions to be a fully-qualified physiotherapist or occupational therapist, and for rehabilitation sessions to last less than 90 min.
The results from this DCE analysis demonstrated that the methodology could be applied in an elderly population in the UK, with a mean age of 79 years, following hip fracture. Only 4 participants did not complete the questionnaire due to lack of understanding, further supporting findings by Milte et al. (8) and Laver et al. (9), who also demonstrated that this method could be used with older adults who had recently experienced hip fracture and other health problems, such as stroke and neurological conditions. The FEMuR feasibility study sample and the DCE sample were predominately female. Participants tended to live alone in properties they owned. The majority of participants were discharged from hospital directly to their usual place of residence, indicating that participants recruited to the FEMuR feasibility study were relatively healthy prior to their hip fracture.
Laver et al. (9) previously explored the differences in preferences of patients and clinicians for rehabilitation service delivery in southern Australia. Similar to the DCE presented in this paper, attributes were based on characteristics of the service (e.g. mode of therapy, dose of therapy and team providing therapy). However, Laver et al. (9) also explored individual outcomes; for example, amount of recovery made and cost of therapy programme. Both the DCE undertaken by ourselves and Laver et al. (9) showed participants found time to be an important factor to patients in rehabilitation.
Milte et al. (8) explored what patients were willing to endure during rehabilitation to improve their mobility, using attributes of: risk of falling; levels of pain; levels of physical effort; and mobility. Findings demonstrated respondents were willing to participate in rehabilitation programmes involving moderate pain and effort in order to improve their mobility. The DCE in this study, and the one conducted in our feasibility study, demonstrated that the method could be used with an older patient population. However, as the DCE carried out by Milte et al. (8) focused on individual characteristics, such as levels of pain, rather than characteristics of the service, such as who delivers the rehabilitation, no further comparisons can be made.
Griffiths et al. (10) found stable mobility, particularly when performing valued activities, for example personal care, day-to-day activities and hobbies, was most important to patients following hip fracture. Since rehabilitation assists in improving mobility and physical function following hip fracture, this DCE can be used to aid service configuration so that the most appealing package of rehabilitation is developed, encouraging patients in their recovery.
To our knowledge, this is the first application of DCE methods to UK older hip fracture patients. Furthermore, the DCE focused on service configuration, rather than individual outcomes for the patient, such as pain. The DCE also assessed preferences for the newly developed intervention of the FEMuR feasibility study, by integrating the workbook into the DCE design. DCEs are reliant on the choice of appropriate and meaningful attributes for their intended audience. The wrong choice of attributes and levels could result in a DCE that is not meaningful to the population, and could lead to incorrect recommendations going forward to policy (17). To reduce the likelihood of this, Abiiro et al. (17) state that attribute development should be systematic, rigorous and transparent. There is growing recognition of different approaches to attribute development in DCEs, including the use of systematic review, expert opinion and qualitative methods such as interviews and focus groups (6, 12). We used multiple methods to develop attributes, including systematic review and findings from focus groups, taking a rigorous and systematic approach to attribute development and design, as championed by others in the field (6, 12, 17), to arrive at meaningful attributes for our participants that can inform policy. The study sample used in this DCE was small; therefore, results should be viewed with caution. This DCE was a pilot, demonstrating the use of the method with a frail, elderly population within a UK setting. The findings from this pilot only provide the views of a small sample (52% of the main study sample). The results are dependent on rehabilitation experiences, and how this particular sample viewed their rehabilitation at the time they were surveyed; therefore, their generalizability may be limited outside these contexts. A dominance test was not included, as none of the profiles generated by the design catalogue were dominant, and an additional question to test for dominance was not included, in order to administer the least burdensome questionnaire to participants. This is a limitation of the study, as the omission of this test meant that consistency of participants’ choices could not be assessed. Scale heterogeneity was also not assessed, due to the small sample size, which is a further limitation of this study. However, the pilot DCE fills a gap in the literature by designing a DCE around service configuration characteristics compared with individual patient outcomes, which have been explored previously (8–10). Furthermore, we feel that by focusing on service configuration this DCE design has the potential to inform service implementation; providing guidance on the components patients prefer, which could be utilized by practitioners when developing and designing services or service guidance. The next steps for this feasibility research would be to determine if the findings can be replicated in a larger scale study. As this analysis did not account for scale and preference heterogeneity it would be useful for further research to use techniques that are able to account for these (18–20). There is also a need for further research to be undertaken in different healthcare contexts. Previous research has been conducted primarily in the UK (10) and Australia (8, 9); therefore, it would be useful to assess whether preferences vary in different cultural contexts, and healthcare systems.
The DCE demonstrated that this method could be used in a UK context, with older hip fracture patients, mean age, 79 years. Participants indicated significant preferences for a fully-qualified physiotherapist or occupational therapist to deliver the rehabilitation, and for rehabilitation sessions to last less than 90 min. As rehabilitation is a part of hip fracture recovery, it is important to deliver a meaningful package to individuals. The design of the DCE using attributes associated with service configuration could have the potential to inform future DCEs in this area, service implementation and assist rehabilitation service design that incorporates the preferences of patients.
The authors would like to thank the patients, carers and staff who took part in the FEMuR feasibility study. The researchers would also like to thank Dr Emily Holmes for providing guidance with regards to DCE analysis. This research was funded by the Health Technology Assessment (HTA) programme of the National Institute of Health Care Research (NIHR) (HTA reference: 11/33/03). The views and opinions expressed are those of the authors and do not necessarily reflect those of the HTA programme, NIHR, the NHS, or the Department of Health.


 Click to show fullsize
Click to show fullsize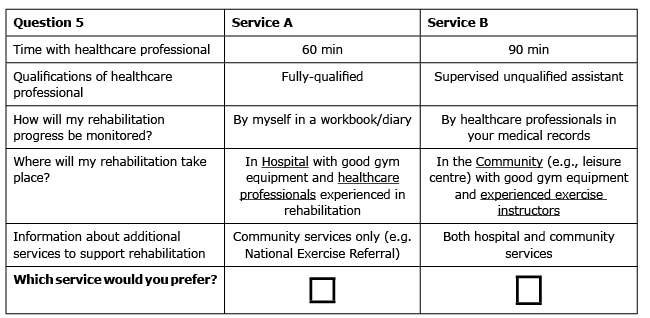 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize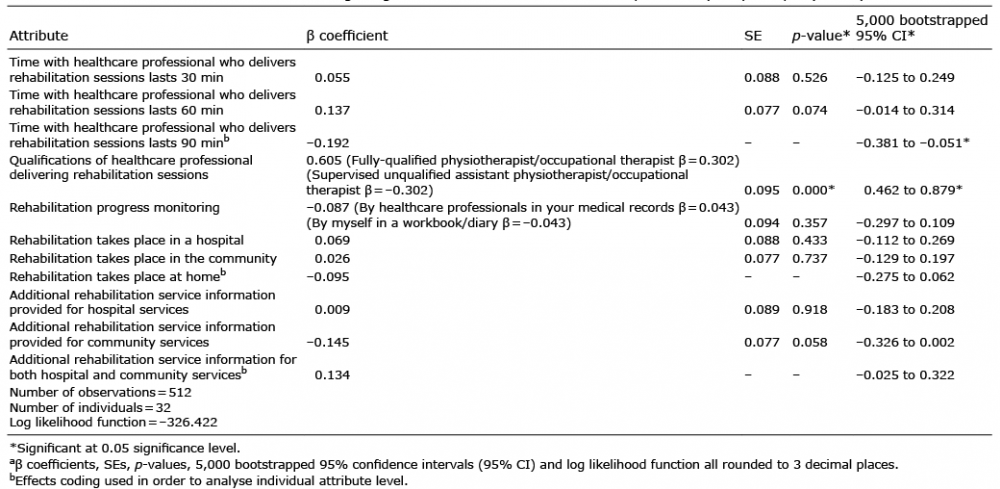 Click to show fullsize
Click to show fullsize